Well, I think there is probably another reason for stem cell research going on elsewhere.
The point is that crucial research is going on in countries with universal health care.
Can you provide some reason to believe that there is about a trillion dollars of adminstrative costs available to be recovered?
You're fixated on the trillion number, I'm not how that was arrived at, but there is a staggering amount of money being burned away in administrative costs in this country:
In 1999, health administration costs totaled at least $294.3 billion in the United States, or $1,059 per capita, as compared with $307 per capita in Canada. After exclusions, administration accounted for 31.0 percent of health care expenditures in the United States and 16.7 percent of health care expenditures in Canada.
http://www.nejm.org/doi/full/10.1056/NEJMsa022033
People are welcome to find more recent numbers. That was a good, clear expression.
Here's a comparison between private insurance and Medicare:
The Federal government usually reports its Medicare administrative costs at about 2% of total payments under the program while private costs vary dramatically from market to market, but frequently are cited to be in the 15-20% range on average.
http://www.cahi.org/cahi_contents/resources/pdf/CAHIMedicareTechnicalPaper.pdf
If we just use those Canadian numbers from 1999 (the gap has grown tremendously since then), and do some quick calculations, $1000 per capita means 1000 X 300,000,000 or $300 billion dollars spent on administrative costs. Given the disparity between Medicare and private insurers, going to Medicare only could easily save $100 to $150 billion annually in administrative costs alone.
This is before dealing with profit and the cost-effectiveness of having a large risk pool.
The Wikipedia article on NIH sas that they account for 28% of biotech research money in the US with the rest coming from private industry.
I was going off old numbers. In the 90's, 55% of the best selling drugs on the market began with NIH grants. 28% is pretty huge, though.
Looking at the raw percentages, however, is misleading. Private groups tend to invest in less experimental drugs, preferring to release something very similar to an existing treatment and sell through advertising. The last decade has seen a depressing slowing of new drugs and treatments reaching the market. Removing some of the profit motive from that industry is likely to result in more daring research and development.
Finally, private companies are allowed to purchase drugs from universities that made discoveries from NIH grants. I would be curious to see a breakdown of what % of private R&D goes to clinical trials and other processes after the patent has been purchased.
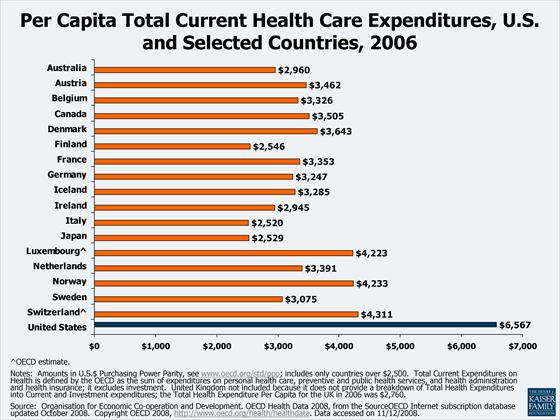
For one thing, most countries are smaller. The cost savings that Canada achieved were somewhere in the neighborhood of 70 billion dollars. The US dropping down to Canada's current per capita takes a trillion dollars out of the picture. That's almost Canada's entire GDP.
If you total the populations and economies of the European nations that have universal coverage, my guess is that you'd be close to an entity the size of the US both in terms of people and size of economy. If Germany-France-England-Switzerland-Scandinavia can do universal health care, I'm not seeing any reason that we can't.
And once again, there are 50 million people (1/6th of the country) on Medicare right now. They are also the most expensive, riskiest population possible, the elderly. If we can provide a single payer system to the riskiest population, which also happens to be a massive group of people, I don't really understand why that can't just be expanded.
And it makes a big difference that for most practical purposes we're the last to do it. When other countries implemented their cost savings there is no guarantee that the money really left the industry. Some, maybe most, of it just got shifted to other countries. If we do it, there's no place left to go, the money will really be out of the industry.
I would like to see you provide some evidence of this international cost shifting.