michaelsuede
Graduate Poster
- Joined
- Mar 21, 2011
- Messages
- 1,565
You do not know ivermectin is safe in Covid-19 until you do the studies. You may guess that because ivermectin is safe pre-Covid-19 when used to treat parasitic infections that it is safe to treat covid-19, but you do not know until the RCT has been done.
if you speculate that covid-19 affects virus-host interactions based on in vitro studies the actual real world impact can only be confirmed by properly planned studies.
There is not a vast body of high quality evidence of the efficacy of ivermectin for covid-19. It disappears as soon as you look at it.
If a properly powered RCT fails to show that there is not a significant effect you can be reasonably sure there is not a significant effect. In clinical medicine, one cannot just count up unpublished papers pro and con, you have to assess the quality power and relevance of studies. High quality, well performed, large studies fail to show an effect. Small, fraudulent, poor quality studies, show unbelievable results. You cannot say 6 terrible non-peer reviewed unpublished papers beat 4 good studies. Anyone who starts an argument in clinical science with the number of studies on one side versus the other has lost.
Anyone who uses an argument based on a fantasy about big pharma influencing the FDA has lost. The NHS easily deals with big pharma. Just look at the number of pharma companies who come to 'confidential' arrangements with the NHS when the NHS refuses to pay the price asked.
If a drug works, it works in a RCT. I do not disagree prospective cohort studies are good trials; but they are as good as RCT not better.
FWI you do the study appropriate to the intervention. For the 'parachute' study you would use a 'play the winner' study not a RCT. There is actually a lot of finesse in clinical research.
Given that billions of doses of ivermectin have been given out during this pandemic with no clear safety signals emerging, I'm pretty sure it's safe for COVID. You got 240 million in Uttar Pradesh getting boxes of this stuff:
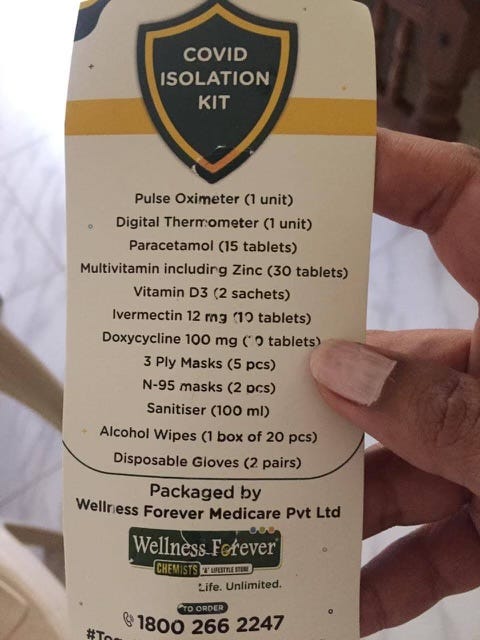
While you continue to harp on RCTs, of which we have several dozen all showing benefit, we also have an entire Indian state wiping out COVID deaths after handing out those COVID kits to everyone.
Epidemiological data should not be dismissed. RCTs are not the end-all-be-all of medical research. I'm positive I could rig an ivermectin RCT to show no benefit by giving out low doses, selective recruitment, only giving it to late stage hospitalized patients, including patients on remdesivir in the ivermectin group but not in the control group, etc.. etc.. RCTs are good, don't get me wrong, but let's not ignore what epidemiology brings to the table.
Last edited:

")